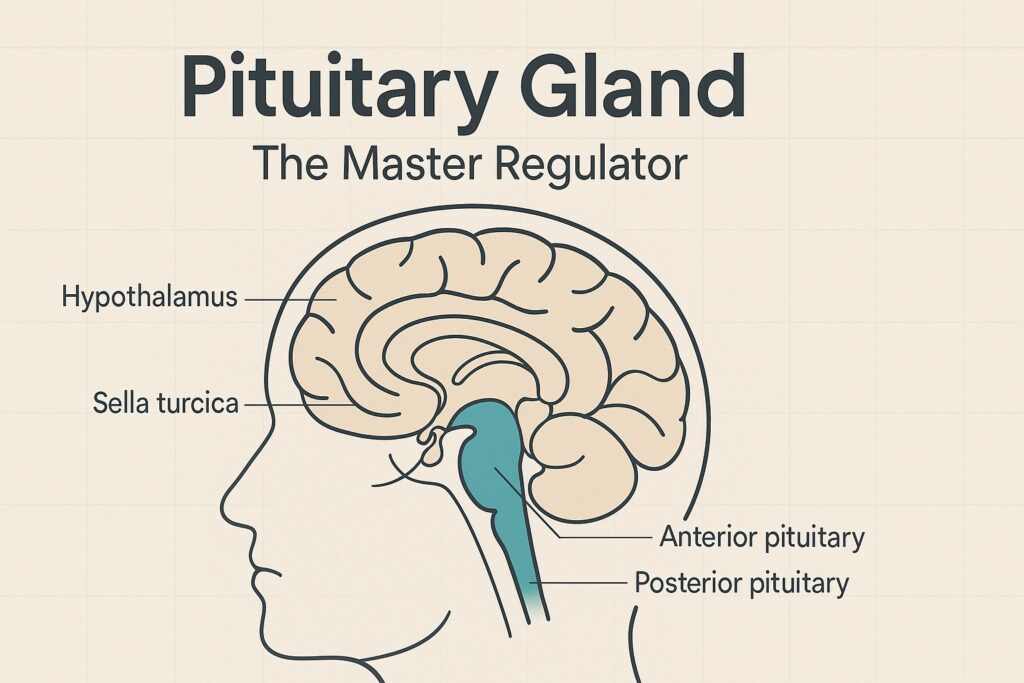
Short answer: the pituitary is the body’s chief endocrine dispatcher. From its seat in the sella turcica at the base of the brain, it releases hormones that keep core processes—growth, stress response, reproduction, lactation, thyroid function, and water balance—within healthy ranges. It does this under minute-to-minute direction from the hypothalamus, using exquisitely tuned feedback loops to maintain homeostasis.
Below is a clear, clinician-level tour of how the pituitary works, what each hormone does, how the system is regulated, and what happens when it goes wrong.
The Command Chain: Hypothalamus → Pituitary → Peripheral Organs
- Hypothalamus samples the internal milieu (temperature, osmolarity, glucose, sleep–wake signals, stress, light) and releases releasing or inhibiting factors into the hypophyseal portal system.
- These signals reach the anterior pituitary (adenohypophysis), instructing it to secrete tropic hormones that act on downstream endocrine glands—or direct-acting hormones that act on tissues.
- The posterior pituitary (neurohypophysis) does not synthesize hormones; it stores and releases the hypothalamic peptides oxytocin and vasopressin/ADH made in the paraventricular and supraoptic nuclei.
- Negative feedback from end-hormones (e.g., cortisol, T3/T4, sex steroids, IGF-1) continuously recalibrates hypothalamic and pituitary output to keep levels in range.
Anterior vs Posterior: Who Makes What?
| Lobe | Hormone (cell type) | Primary Targets | Core Functions |
|---|---|---|---|
| Anterior | ACTH (corticotroph) | Adrenal cortex (zona fasciculata/reticularis) | Stimulates cortisol (stress response, BP support, glucose mobilization) and adrenal androgens. Note: Aldosterone is regulated mainly by RAAS and serum K⁺, not ACTH. |
| TSH (thyrotroph) | Thyroid follicular cells | Drives T3/T4 synthesis → basal metabolic rate, thermogenesis, growth, neurodevelopment. | |
| GH (somatotroph) | Liver, bone, muscle, adipose | Stimulates IGF-1 production (linear growth, protein synthesis), lipolysis; modulates glucose homeostasis. Secreted in pulses, largest during slow-wave sleep. | |
| Prolactin (lactotroph) | Mammary gland | Milk production; tonically inhibited by dopamine. | |
| FSH (gonadotroph) | Ovarian granulosa / testicular Sertoli | Follicular maturation, estradiol synthesis; spermatogenesis support (inhibin-B feedback). | |
| LH (gonadotroph) | Ovarian theca / testicular Leydig | Ovulation, luteinization, progesterone; testosterone production. | |
| Posterior | Oxytocin | Uterus, breast myoepithelium | Uterine contractions, milk ejection; pulsatile release with nipple stimulation; positive feedback during labor. |
| Vasopressin (ADH) | Kidney collecting duct (V2); vessels (V1) | Water reabsorption via aquaporin-2 insertion; vasoconstriction at higher levels; regulated by plasma osmolality and effective arterial volume. |
The Pituitary’s “Main Function,” Expanded
- Homeostatic Control via Axes
- HPA axis: CRH → ACTH → cortisol; buffers stress, maintains blood pressure and glucose, tempers inflammation.
- HPT axis: TRH → TSH → T3/T4; sets cellular metabolic pace.
- HPG axis: GnRH → LH/FSH → sex steroids/gametes; controls puberty, fertility, bone density, body composition.
- GH/IGF-1 axis: GHRH/ghrelin ↑ and somatostatin ↓ → GH → IGF-1; drives stature, tissue repair, and body composition.
- Lactotroph axis: Dopamine (from hypothalamus) suppresses prolactin; suckling and estrogen lift that brake for lactation.
- Water balance: Osmoreceptors/baroreceptors regulate ADH for precise control of serum sodium and tonicity.
- Set-Point Management
- Like a thermostat, pituitary output rises when an end-hormone is low and falls when it is high, maintaining narrow biochemical set-points essential for survival and performance.
- Physiologic Rhythms
- Many pituitary outputs are pulsatile and circadian (e.g., early-morning ACTH/cortisol peak; nocturnal GH surge). These rhythms optimize tissue sensitivity and minimize receptor desensitization.
How Each Hormone Works—Key Details & Clinical Pearls
ACTH (Adrenocorticotropic Hormone)
- Stimulus: CRH, stress, hypoglycemia; inhibition: cortisol feedback.
- What it does: Promotes adrenal cortisol synthesis via POMC-derived ACTH; beta-endorphin and MSH are co-products of POMC processing.
- Why it matters: Deficiency → adrenal crisis (hypotension, hyponatremia, hypoglycemia). Excess (ACTH adenoma) → Cushing’s disease.
TSH (Thyroid-Stimulating Hormone)
- Stimulus: TRH (↑ in cold); inhibition: T3/T4 feedback, dopamine, glucocorticoids.
- What it does: Upregulates NIS (iodide pump), thyroglobulin, TPO; trophic to thyroid.
- Clinical: High TSH + low free T4 = primary hypothyroidism; low TSH + high free T4 = hyperthyroidism. Central (pituitary) hypothyroidism shows low/normal TSH with low free T4.
GH (Growth Hormone)
- Stimulus: GHRH, sleep, exercise, hypoglycemia, fasting (ghrelin); inhibition: somatostatin, hyperglycemia.
- Actions: Via IGF-1 (linear growth, cartilage proliferation); direct anti-insulin effects (lipolysis, ↓ glucose uptake).
- Clinical: Childhood deficiency → growth failure; adult deficiency → ↓ muscle mass, ↑ fat, low energy. Excess → gigantism (children) / acromegaly (adults) with cardiometabolic risks.
Prolactin
- Baseline control: Dopamine tonically inhibits. TRH and estrogen can raise PRL.
- Actions: Mammogenesis, lactogenesis; suppresses GnRH → can cause amenorrhea and galactorrhea when elevated.
- Clinical: Most common functioning pituitary tumor = prolactinoma; first-line therapy is dopamine agonists (cabergoline > bromocriptine).
FSH & LH (Gonadotropins)
- Control: Pulsatile GnRH; pulse frequency and amplitude determine LH vs FSH dominance. Prolactin excess or severe stress suppresses GnRH.
- Women: Folliculogenesis, estrogen production (FSH); LH surge triggers ovulation and luteal progesterone.
- Men: FSH → Sertoli support of spermatogenesis; LH → Leydig testosterone.
- Clinical: Hypogonadotropic hypogonadism (low/normal LH/FSH) vs hypergonadotropic (high LH/FSH with gonadal failure). Kallmann syndrome presents with delayed puberty + anosmia.
Oxytocin (Posterior)
- Triggers: Nipple stimulation, cervical stretch; conditioned by infant cues.
- Actions: Milk let-down, labor contractions; positive feedback loop during parturition.
- Clinical: Used exogenously to augment labor or manage postpartum hemorrhage (uterine atony).
Vasopressin / ADH (Posterior)
- Regulation: Plasma osmolality (very sensitive) and arterial volume/pressure (less sensitive but dominant in hypovolemia).
- Receptors: V2 (renal water reabsorption via aquaporin-2); V1 (vasoconstriction).
- Clinical: Deficiency → central diabetes insipidus (polyuria, polydipsia; treat with desmopressin). Excess (paraneoplastic, CNS disease, drugs) → SIADH (hyponatremia).
The Pituitary in Clinical Practice
Common Pituitary Disorders (What to look for)
| Disorder | Pathophysiology | Notable Features | First-line Management |
|---|---|---|---|
| Prolactinoma | Lactotroph adenoma → PRL excess | Galactorrhea, hypogonadism, infertility | Cabergoline (dopamine agonist) |
| Acromegaly | Somatotroph adenoma → GH excess | Enlarged hands/feet, jaw growth, OSA, cardiomyopathy | Transsphenoidal surgery; somatostatin analogs, pegvisomant |
| Cushing’s disease | Corticotroph adenoma → ACTH excess | Central obesity, striae, HTN, glucose intolerance | Surgery; medical therapy if not cured |
| Nonfunctioning adenoma | Mass effect without hormone excess | Headache, bitemporal hemianopsia, hypopituitarism | Surgery if compressive; hormone replacement |
| Hypopituitarism | Tumor, apoplexy, Sheehan syndrome, irradiation | Sequential loss: GH → gonadotropins → TSH → ACTH | Replace in physiologic order (steroids before thyroid) |
| Pituitary apoplexy | Acute hemorrhage/infarct of adenoma | Sudden headache, visual loss, ophthalmoplegia, shock | High-dose steroids, urgent neurosurgical eval |
| Sheehan syndrome | Postpartum pituitary infarction | Failure to lactate, amenorrhea, fatigue, hypotension | Lifelong hormone replacement |
Pregnancy physiology: Estrogen-driven lactotroph hyperplasia enlarges the gland by up to 30%; PRL rises. A large macroadenoma may become symptomatic in pregnancy—hence the need for preconception planning.
How We Test the Pituitary
- Baseline labs (screening):
- Morning cortisol, TSH/free T4, PRL, IGF-1, LH/FSH with estradiol (women) or total testosterone (men), sodium/osmolality if water balance suspected.
- Dynamic tests (reserve):
- Insulin tolerance test (gold standard for GH and ACTH reserve), cosyntropin stimulation (adrenal axis), glucagon or arginine tests (GH), water deprivation or hypertonic saline/copeptin for DI/SIADH differentiation.
- Imaging:
- Pituitary MRI with gadolinium for adenomas, stalk lesions, empty sella, apoplexy.
Therapeutic order matters: In combined deficiency, always replace glucocorticoids before thyroid hormone to avoid precipitating adrenal crisis.
Practical Physiology Nuggets & Clarifications
- Aldosterone control: chiefly angiotensin II and serum potassium; ACTH provides only transient support.
- Prolactin regulation: unique in that it is suppressed—not stimulated—by a hypothalamic factor (dopamine).
- GnRH physiology: continuous GnRH suppresses LH/FSH (used therapeutically in endometriosis/prostate cancer); pulsatile GnRH is required for fertility.
- GH rhythm: secretion is pulsatile and rises during puberty; highest single pulses occur soon after sleep onset.
- Circadian ACTH/cortisol: peaks before waking; shift work, depression, and chronic stress can blunt or distort this rhythm.
So—What Is the Pituitary’s Main Function?
To maintain homeostasis by acting as the central endocrine relay:
- It translates hypothalamic signals into targeted hormonal commands.
- It coordinates downstream glands (thyroid, adrenals, gonads) and directly modulates growth, lactation, and water balance.
- It stabilizes vital set-points through continuous feedback and rhythmic secretion aligned with sleep, nutrition, stress, and environmental cues.
When the pituitary is healthy, the body’s internal economy remains balanced: energy is available when needed, growth unfolds on schedule, reproduction is possible, and water–electrolyte balance keeps the brain safe. When it falters, the consequences are multisystemic—one reason the pituitary is rightly called the body’s master gland.
Key Takeaways
- The pituitary’s primary function is homeostatic regulation via hormone release that coordinates stress response, metabolism, growth, reproduction, lactation, and water balance.
- The anterior lobe produces six classic hormones (ACTH, TSH, GH, PRL, FSH, LH); the posterior lobe releases hypothalamic oxytocin and ADH.
- Feedback loops (HPA, HPT, HPG, GH/IGF-1) and neural reflexes (suckling for PRL/oxytocin; osmoreception for ADH) keep physiology within tight bounds.
- Understanding the pituitary’s axes is essential for recognizing and treating disorders from Cushing’s and acromegaly to prolactinomas, diabetes insipidus, and hypopituitarism.